Ask A Researcher
April 2017
A Brief Introduction to the North Dakota Pregnancy Risk Assessment Monitoring System (PRAMS)

Grace Njau is the Principal Investigator of the North Dakota Pregnancy Risk Assessment Monitoring System (PRAMS). She also serves as the Maternal/Child/Oral Health Epidemiologist at the North Dakota Department of Health. Grace received her master’s degree at the University of Colorado in 2014 and is currently a doctoral student at the University of Tennessee. Grace is passionate about perinatal research and all-things-data, especially rapid and targeted data dissemination to inform policy and program planning.
Acknowledgements
North Dakota Pregnancy Risk Assessment Monitoring System (PRAMS) is a joint research project between the state departments of health and the Centers for Disease Control and Prevention (CDC). It is funded by the CDC and is headed by staff from North Dakota Department of Health’s (NDDoH) Maternal and Child Health Program in partnership and contract with Center for Social Research at North Dakota State University (NDSU), American Indian Public Health Resource Center at NDSU, and the Tribal Nations Research Group at Turtle Mountain Band of Chippewa Indians. The activities and priorities of ND PRAMS are shaped by a Steering Committee consisting of maternal and child health experts, stakeholders and tribal partners. To-date, ND PRAMS has received tribal approval and support from Turtle Mountain Band of Chippewa Indians and the Mandan-Hidatsa-Arikara Nation. North Dakota PRAMS is also partnering with the Great Plains Tribal Chairmen’s Health Board which will be conducting a parallel tribal PRAMS at Standing Rock and Lake Traverse Reservations.
Background
According to the CDC’s PRAMS Working Group, PRAMS is an “ongoing, population-based surveillance system designed to identify and monitor selected maternal experiences and behaviors that occur before and during pregnancy and during the child’s early infancy among a stratified sample of women delivering a live birth”. Its inception in 1987 aimed at assisting state health departments to establish and maintain a systematic surveillance system of new mothers’ select risk factors and outcomes. This was especially important at the time since there was a stall in the decline of low birth weight infants being born as well as minimal improvement in infant mortality, despite significant advances in maternal and fetal medicine, and neonatology. Through a standard protocol, PRAMS is designed to supplement data from vital records and to generate data for program planning and evaluation of early infancy programs. The overall goal of PRAMS is to “reduce infant morbidity and mortality and to promote maternal health by influencing maternal and child health programs, policies, and maternal behaviors during pregnancy and early infancy”, according to the PRAMS Working Group.
In 2002 North Dakota was selected to conduct a Point-in-Time PRAMS study by the CDC. In 2016 the ND Department of Health again applied for a more long-term PRAMS study. North Dakota was selected as a PRAMS site and data collection is to be initiated in April of 2017. This five-year cooperative agreement with the CDC involves the collection, analyses and dissemination of maternal and early infancy data on the health, behavioral and social risk factors of new mothers before, during and after pregnancy. The ND PRAMS research project aims to:
1. Utilize the CDC model protocol to effectively collect, analyze, and disseminate timely and highly-scientific quality data on maternal risk factors, behaviors, and attitudes relating to pregnancy and early infancy that will result in translational efforts that reduce adverse maternal and infant outcomes.
2. Foster partnership and culturally-competent data collection, analyses and dissemination practices within ND communities, including American Indian communities, in efforts to adequately monitor risk factors that can be modified to improve and minimize disparities in maternal and infant health.
The purpose of ND PRAMS is to supplement vital records data regarding maternal behaviors and experiences. As of 2017, no alternate data sources are available in ND to measure the current prevalence of the topics below – making PRAMS a valuable addition to maternal and child health data capacity in the state:
- ND-specific American Indian tribal affiliation
- Safe sleep practices
- Folic acid consumption among women during pregnancy
- Utilization of and access to dental services during pregnancy
- Barriers to breastfeeding initiation and continuation
- Maternal utilization of family planning services
- Utilization of progesterone in women with a previous preterm birth
- Maternal ACEs through supplemental ND-added PRAMS questions
- Reach of the Child Passenger Safety and Newborn Screening Programs
- Medical marijuana use
- Substance use and abuse
Significance of the project
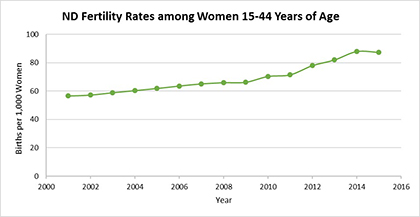
At an estimated 757,952 residents by the U.S Census Bureau in 2016, North Dakota experienced the highest percentage growth of all states from 2010 to 2016, with a 13 percent population increase. Fertility rates in the state for women between the ages of 15 and 44 have followed similar trends indicating an over 50 percent increase in the number of births per 1,000 women between 2001 and 2015, as shown below.
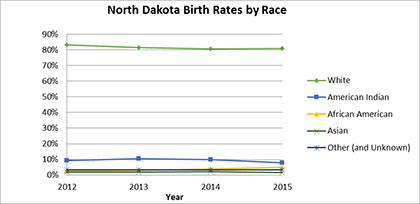
In 2015, there were 12,842 births occurring in ND. Of those births, 11,011 births were to ND residents (resident births). Approximately 81 percent of the resident births in 2015 were to mothers between the ages of 20-35 years and 97 percent of births were singleton deliveries, according to ND Division of Vital Records. The racial diversity of births in the state continued to increase with White births being the majority at 80 percent, followed by American Indian births at 9.7 percent. African American births accounted for 5.0 percent of all resident births – representing a 74 percent increase from 2014. All other races accounted for 4.3 percent of all the births. Hispanic births in the state also increased by 51 percent since 2014 and in 2015, accounted for about 6 percent of all births in the state.
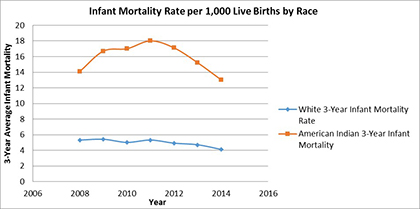
As the population grows, ND continues to face various challenges in the maternal and child health population. For example, while the overall infant mortality in the state averages at about 6 infant deaths per 1,000 live births, the infant mortality rate among American Indian births (12.9 per 1,000) is more than double that of the White population at 5.1 infant deaths per 1,000 live births. The infant mortality rate for ND American Indians is also significantly higher than the national American Indian infant mortality rate of 8.1 per 1,000 live births. Birth defects, prematurity, low birth weight and Sudden Infant Death Syndrome are the leading causes of death in ND infants. While these causes of infant death are fairly consistent with national causes of death, ND had a higher rate of birth defects at 138.9 per 100,000 compared to the national rate of birth defects of 124.7 per 100,000 live births on average between 2011 and 2013.
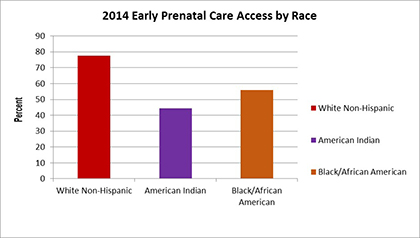
Between 2011 and 2013, the average rate of preterm birth (births at less than 37 weeks gestation) was 9.9 percent of all live births. While this rate was lower than the national average rate of 11.6 percent, disparity by maternal race was evident, especially in the American Indian populations with the average rate of preterm birth being 15.1 percent between 2011 and 2013, compared to the White population preterm birth rate of 9.2 percent. This American Indian rate of preterm birth in ND was also higher than the national rate of American Indian preterm births (13.3%). Additionally, while the rate of mothers getting adequate prenatal care remained fairly steady ranging from 82.5 in 2010 to 81.2 in 2015; American Indian women were the lowest proportion of women receiving early prenatal care at 44 percent compared to 75 percent of White mothers.
Smoking during pregnancy is also a cross-cutting challenge with approximately 13.8 percent of ND mothers reporting smoking at any point during pregnancy in 2015. Additionally, in 2016, ND became one of 28 states to legalize the use of medical Marijuana, of which no state has been able to adequately assess its impact to the maternal and child health population.
ND PRAMS Research
The questionnaire that will be used has two types of questions, those which must be asked by all participating states, and state-specific questions. In shaping the ND PRAMS specific questions for the questionnaire, the Steering Committee took into consideration 1) the areas where the state had no alternate data sources, 2) emerging issues in the state, and 3) the risk factor areas in which the state has not been showing improvements. This led to the inclusion of questions on topics such as prenatal care access barriers, maternal substance abuse, oral health care barriers, Adverse Childhood Experiences (ACEs), among others.
To adequately study and describe the risk factors and disparities described within the state’s maternal and child population, ND PRAMS will oversample American Indian mothers when administering the survey. This oversample will also allow for tribes to receive data from their own communities to inform practice and planning.
Given the success of the 2002 North Dakota Point-in-Time PRAMS that had a 73 percent overall response rate, in planning for the PRAMS data collection that will begin in April 2017, ND PRAMS program staff are counting on the strong partnerships established with the local and state partners to build up and sustain momentum for the program.
The data collected over the course of ND PRAMS will be instrumental in creating and sustaining programs that will help improve the well-being of all babies, mothers, and families in North Dakota. We look forward to having North Dakota mothers share their story!
For more information on PRAMS please contact Grace Njau at
North Dakota Pregnancy Risk Assessment Monitoring System (ND PRAMS)
Division of Family Health |North Dakota Department of Health
600 E Blvd Ave, Dept 301 |Bismarck, ND 58505-0200
Email: gnjau@nd.gov |Office: 701.328.3209.
Center for Social Research
North Dakota State University
Compass created by:
Wilder Research
© 2025. All rights reserved.